

Jul 22, 2026
_Artboard%201.png)
Aug 12, 2022
- Share on:




-
 copied
copied
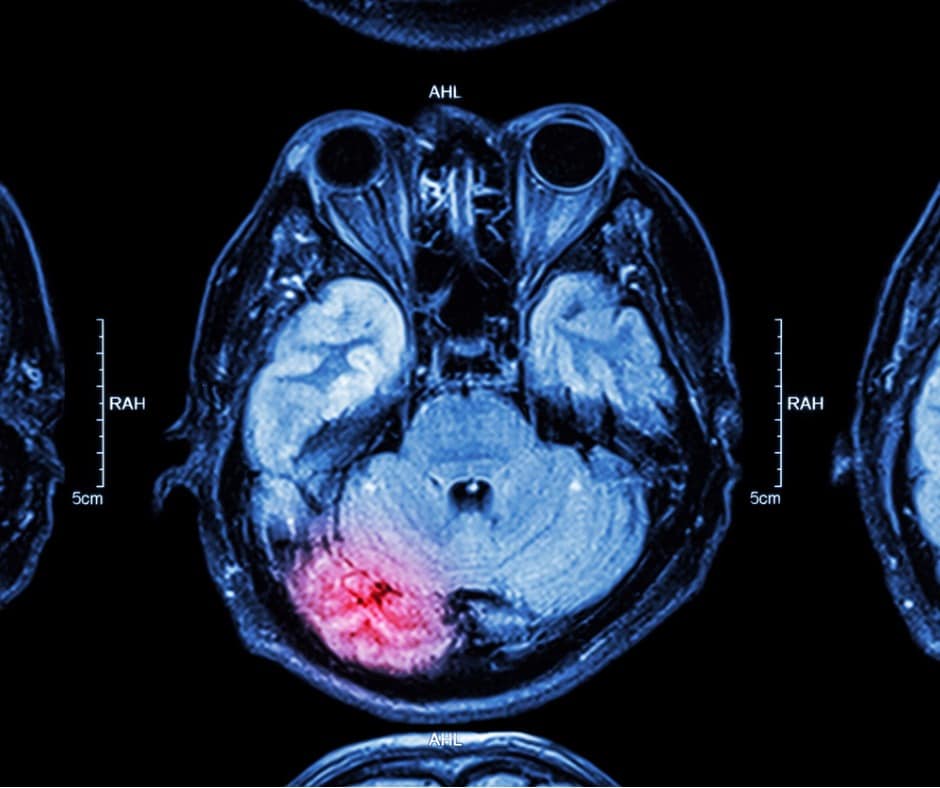
Cerebral Infarction Definition
A cerebral infarction is an ischemic stroke that results from a blockage or narrowing in the blood vessels that supply blood and oxygen to the brain.
Causes and Coding for Cerebral Infarction
The causes for cerebral infarction include thrombus, embolism, or stenosis. Coding of cerebral infarction provides many challenges as the codes are specific to site and there are many different arteries that may be the culprit that fall within category I63- Cerebral infarction. It is pertinent that the coder reviews the medical record documentation for further specificity of the cerebral infarction. This can be found by reviewing radiology records, consultations, progress notes and other physician documentation.
Hemorrhagic
A hemorrhagic conversion or transformation often complicates a cerebral infarction/ischemic stroke. This is due to many different causes one of which is tPA administration for treatment of the cerebral infarction/ischemic stroke. Codes from Categories I60-, I61-, and I62- would be reported for the intracerebral, intracranial, or subarachnoid hemorrhage identified. Again, it is pertinent to review the medical record documentation to ensure that the most specific site of hemorrhage is coded.
Both the cerebral infarction (be sure and look for specificity in the diagnosis) and the cerebral hemorrhage should be reported when present. There are no Excludes1 notes when reporting codes for both these conditions. There are also many AHA Coding Clinics that advise both codes should be reported.
Authored by Kim Boy, RHIT, CDIP, CCS, CCS-P
References:
AHA Coding Clinic, Second Quarter 2017, Page: 9-10
AHA Coding Clinic, Third Quarter 2010, Page 5-6
AHA Coding Clinic, Third Quarter 2007, Page 4
wikipedia.org/wiki/Cerebral_infarction
ncbi.nlm.nih.gov/pmc/articles/PMC3677128/
HIA’s comprehensive auditing approach includes acute coding audits and Clinical Documentation Integrity (CDI) audits.

The information contained in this coding advice is valid at the time of posting. Viewers are encouraged to research subsequent official guidance in the areas associated with the topic as they can change rapidly.
Need to Earn CEUs?
Our coding education platform, HIAlearn.com, offers courses related to this topic and many more. Subscribe today and access more than 230 courses accepted by AHIMA for CEUs, with a selection also accepted by AAPC.

