

Jun 24, 2026
_Artboard%201.png)
Dec 13, 2019

- Share on:




-
 copied
copied
Changes in Cardiac Catheterization Code Descriptions and Reporting
With the implementation of ICD-10-PCS the description of codes became much more detailed to describe exactly what is being performed. Cardiac catheterization is one of the descriptions that changed to further detail exactly what is being performed during the procedure.
In ICD-9, the description of the codes reported for the heart catheterizations were: 37.22-Left heart catheterization; 37.21-Right heart catheterization; and 37.23-Combined right & left heart cardiac catheterization. This was difficult to code because physicians were documenting that they were performing a left and/or right cardiac catheterization, without full understanding of what is needed to report these procedures.
- 4A023N7—Measurement of cardiac sampling and pressure, left heart, percutaneous approach
- 4A023N6—Measurement of cardiac sampling and pressure, right heart, percutaneous approach
- 4A023N8—Measurement of cardiac sampling and pressure, bilateral, percutaneous approach
ICD-10-PCS has taken away the misunderstandings that were being seen, by changing the description of the ICD-10-PCS codes to truly fit the procedure that is being performed. The description now states that a measurement is taken.
As you can see, all of these now require measurement in order to be reported.
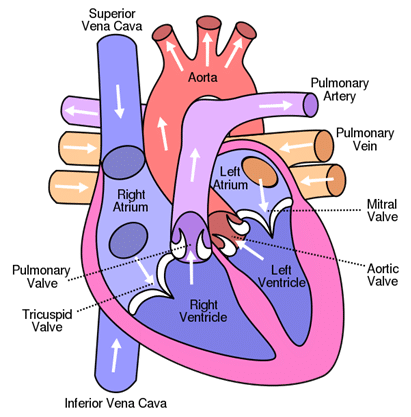
Photo courtesy Wikimedia
Note: There are also multiple definitive procedures that may be performed during a cardiac catheterization but this coding tidbit is focusing on the diagnostic aspects.
What is a Cardiac Catheterization?
A cardiac catheterization is a procedure performed to diagnose or treat certain cardiovascular conditions. Small catheters are inserted into blood vessels to obtain x-ray pictures of the coronary arteries and cardiac chambers. The catheters are put into a blood vessel in your arm, neck or groin/upper thigh. The entry site of the catheter does not impact the ICD-10-PCS code. During cardiac catheterization, pressures may be measured for intra-cardiac hemodynamics which show the blood flow in the heart or even take samples of blood or biopsy of heart muscle.
Diagnostic Left Heart Catheterization includes: the left atrium, ventricle, the mitral and aortic valves, the ascending left aorta and possible the pulmonary veins.
Diagnostic Right Heart Catheterization includes: the right atrium, ventricle, tricuspid and pulmonary valves, the main pulmonary branches and superior and inferior vena cava.
Diagnostic Combined Heart Catheterization includes: a single procedure which includes the evaluation of both the left and right as above.
Common Diagnostic Procedures Performed During Cardiac Catheterization
Coronary angiography
—oftentimes performed during a diagnostic cardiac catheterization to check for blockages in the arteries of the heart. Dye is injected through the catheter and special x-ray images are taken of the heart as the dye moves through the heart chambers, valves and major vessels. The type of contrast used for the angiography must be known in order to accurately report the appropriate ICD-10-PCS code. This procedure may be completed with or without a diagnostic heart catheterization. The reason for this is that the coronary arteries branch off of the aorta just before the heart and aortic valve. In order to report a diagnostic left heart catheterization, the aortic valve must be crossed with the catheter and LV pressures for hemodynamics obtained.
Ventriculogram
—performed to evaluate ventricle contraction and blood flow in the heart. This test is performed to diagnose or assess heart valve issues and is also a test that measures the ejection fraction of the heart. Contrast is injected into the heart’s ventricle(s) to measure the volume of blood being pumped. If a ventriculogram is performed during a left heart catheterization, the catheter is moved through the aortic valve into the left side of the heart. If a ventriculogram is performed during a right heart catheterization, the catheter is moved into the right side of the heart in order to record pressures from the right atrium and right ventricle.
Intravascular ultrasound (IVUS)
—performed via an ultrasound catheter with ultrasound capabilities to record pictures of vessels evaluated. This allows the physician to see and measure the inside of the blood vessels.
Fractional flow reserve (FFR)
—guidewire based procedure that can accurately measure blood pressure and flow through a specific part of the coronary artery. This test helps the physician determine if a vessel is amenable to angioplasty or stenting.
Coding Tips for Reporting Left and Right Heart Catheterizations
- Know the common abbreviations used during cardiac procedures
- Look for pressures in the procedure note: LV pressures (mm/hg) should be documented when a left heart catheterization is performed; RV pressures should be documented when a right heart catheterization is performed. Remember that pressures must be documented in order to report in ICD-10-PCS.
- If the pressures are not in the procedure note, coders oftentimes find them in the procedure event log or “run sheet” and it is appropriate to look here
- In order to report a left heart catheterization, the catheter must cross the aortic valve
- Coronary angiography may be completed without a true left heart catheterization because the coronary arteries branch off of the aorta just before the aortic valve
Authored by Kim Boy, RHIT, CDIP, CCS, CCS-P
References
heart.org/en/health-topics/heart-attack/diagnosing-a-heart-attack/cardiac-catheterization
mayoclinic.org/tests-procedures/cardiac-catheterization/about/pac-20384695
hopkinsmedicine.org/health/treatment-tests-and-therapies/cardiac-catheterization
clevelandclinic.org/health/diagnostics/16832-cardiac-catheterization/test-details
http://commons.wikimedia.org/wiki/Heart
For more information on coding cardiac catheterizations and associated diagnostic and definitive procedures, please check out our course on this subject.
In need of coding support? We offer both inpatient coding support and outpatient coding support services. Partner with us to replace underperforming coding vendors, get coding backlogs caught up, staff for a FMLA/vacation gap, special projects, to assist in Single Path Coding, or for Total Outsource Coding Support.

The information contained in this coding advice is valid at the time of posting. Viewers are encouraged to research subsequent official guidance in the areas associated with the topic as they can change rapidly.
Need to Earn CEUs?
Our coding education platform, HIAlearn.com, offers courses related to this topic and many more. Subscribe today and access more than 230 courses accepted by AHIMA for CEUs, with a selection also accepted by AAPC.

